Special Cases
Mandibular anterior teeth
From an esthetic standpoint, the mandibular veneer can provide an excellent result in most situations. However, its life expectancy can be drastically compromised unless the patient’s occlusion is favorable.
The usual problem with preparations for lower veneers is leaving enough tooth structure remaining after the horizontal and vertical reduction. A potentially weak point is at the inciso-labial junction, which must always be sufficiently reduced and rounded to allow the veneer to be thick enough in that area to have the strength to resist fracturing when placed under an occlusal load. Also, the incisal edge of the mandibular anterior teeth is usually the most visible part of the veneer so consider this fact when preparing the tooth. Sufficient incisal reduction is needed to ensure a normal incisal edge appearance for that patient.
One advantage of the mandibular veneer is that it is seldom necessary to go subgingivally, as with the maxillary veneer, because most people do not show the gingival margin of mandibular anterior teeth.
To reduce or not?
The most practical approach is to evaluate each patient, and indeed each tooth to be veneered, on the basis of:- the thickness of the veneer needed for covering or reshaping,
- the degree of anticipated retention of the veneer, considering the receptivity of the tooth to the bonding agent and placement of the veneer, and
- recognition of how the increased thickness of the veneered tooth will change its appearance, structure, alignment, and function.
Dark abutments
Tooth darkening represents a major challenge for the restoration of optical characteristics with the naturalness of adjacent teeth as a reference. The amount of tooth reduction is determined by the color of the substrate.
In this case, the alternatives for establishing a good result are;
- performing a more invasive preparation,
- using opacifiers before the impression taking,
- selection of less translucent ceramic, with sufficient masking capability
- use of more opaque and/or higher value resin cement,
- also the combined use of the aforementioned alternatives.
Conceptually, the rehabilitation of darker teeth requires greater preparation depth; however, the challenge of conservatism is to remove a minimal amount of tooth structure and at the same time avoid the risk of inadequate tooth reduction for the proposed ceramic restoration. Until recently, severely discolored teeth represented a situation of contraindication for veneers. However, the improvement of ceramic systems and the association of new ingots with higher control of light transmission have enabled performing more conservative techniques as well as build-ups on discolored substrates with an increasingly more natural result.
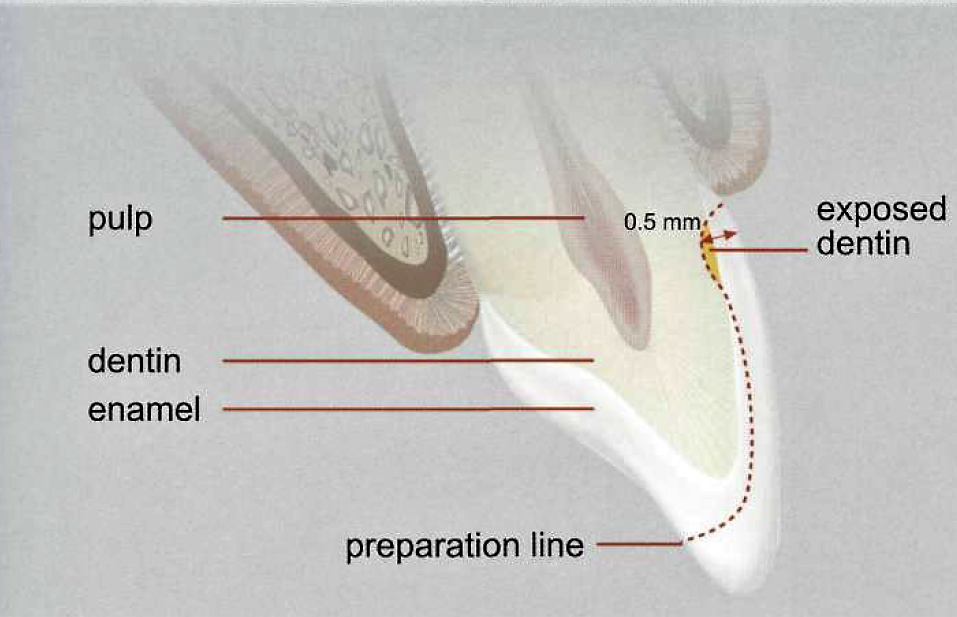
Darkly stained teeth often require more reduction for opaquing purposes. This will allow for a thicker, more opaque veneer. For veneers on tetracycline‐stained teeth, for example, the underlying tooth color will modify its shade dramatically. This is because, in most cases, the veneer is only 0.5 mm thick and rather translucent. As a result, the actual shade of the porcelain has only a nominal influence on the final color of the bonded veneer.
With teeth darkened by endodontic treatments in which the labial surface is intact and the rehabilitation of which will maintain the natural morphology, the silicone guide may be fabricated directly within the mouth and prior to preparation.
The darker the abutment, the more reduction we have to do ..
 |
| Generally speaking, a depth of 0.2 mm is needed to change the hue of the tooth by one shade. |
By reducing the tooth, usually it will be possible to neutralize the underlying color and create the illusion of a normal tooth color by having the opaque incorporated into the veneer itself. Also, by making room for the application of opaquing layers under the veneer, additional opaquing can be obtained at the cementation appointment by using resin opaquers.
Wherever possible, the use of ceramic veneers on discolored substrates needs to provide a balance between its capacity to mask the substrate and the final aesthetic result. Increased thickness of the restoration and the use of a lower translucency ceramic collaborate with the masking. However, increased thickness necessarily means more invasive tooth preparation, which reduces the amount of enamel available for bonding procedures, thus decreasing the clinical success expected for the porcelain veneer.
Currently, the dental market makes available a range of ceramic systems with different degrees of translucency, suitable for the manufacture of ceramic veneers. Excessively opaque ceramics such as IPS e.max, MO (medium opacity), and HO (high opacity) (Ivoclar Vivadent, Liechtenstein) are incapable of simulating the optical behavior of tooth enamel, which is characterized by its translucency, lending to restorations an artificial, unsightly appearance. Although MO ingots are still offering good results.
Hilgert studied the ability of ceramic veneers to mask discolored backgrounds in an aesthetically acceptable manner with decreased biological cost, concluded as follows:
- For non-discolored substrates, such as A1 (Vita Classical® shade guide, Vita, Germany), high translucency ceramic systems with a thin thickness may be reliably utilized (0.4 mm) - Empress Aesthetic® HT (Ivoclar Vivadent, Liechtenstein) and IPS e.max HT (Ivoclar Viva-dent, Liechtenstein).
- Slightly discolored substrates (A3.5 VitaClassical® shade guide, Vita, Germany) were masked acceptably with a conservative preparation (0.4 mm reduction) if associated with low translucency ceramics (EmpressCAD® LT, Ivoclar Vivadent, Liechtenstein).
- Severely discolored substrates (C4, VitaClassical® shade guide, Vita, Germany) were restored acceptably by merely executing an invasive preparation (1.0 mm) and low translucency ceramics (EmpressCAD® LT, Ivoclar Vivadent, Liechtenstein).
Aged teeth
This has been an aspect of veneer preparation often ignored or overlooked until now, but it becomes an important issue when this application is performed over facially eroded or aged teeth. These teeth, owing to the thinning of the existing enamel surface, have already lost their original facial volume and have become weakened. If this is not taken into account, the ignorant application of the depth cutter will be extremely destructive, resulting in the total loss of the existing thin enamel surface.
It is vitally important to respect the thickness of the enamel that remains during teeth preparation as well as the biomimetic recovery of the crown and the original enamel thickness. When these principles are followed, the healthy tooth structure is preserved because if the teeth are overprepared, nothing can replace the unnecessarily lost healthy tooth structure resulting in the loss of the enamel which is the source of the strength of the teeth. This has always created a problem during the preparation of aged teeth for ceramic veneers. The final forms and contours of the teeth can also be accomplished during the provisionalization phase.
During the natural aging process, the enamel thickness of the aged teeth gets thinner and thinner, gradually losing its original volume.
The thinner the enamel, the more flexible the tooth becomes ..
Therefore the dentist must try his/her hardest to preserve as much of the existing enamel as possible. This is one of the most important situations where the APT must definitely be utilized. If the APT is not used, at least a silicon index (prep. guide) prepared over the wax-up should be utilized. It will dictate the final volume and hence inform the dentist about the depth already lost to facial erosion. In this way, the maximum conservation of the enamel will be achieved. On the other hand, if a solid reference such as a silicone index is not used, the extreme preservation of enamel thickness during tooth preparation often leads to overcontouring of the final restorations.
Crowded teeth
Preparation of crowded teeth also needs a preplanned, delicate approach, especially if the mandibular incisors are of concern. Since some special cases need more aggressive preparation depths, such as in the case of the discolored or facially misaligned teeth, reduction of the facial surface on the teeth that suffer from severe discoloration must not be limited to the enamel. The preparation will have to be deeper, even if it exposes the dentin. Whenever it is feasible, increasing the depth of reduction to 0.5 mm in the cervical region and 0.7 mm in the middle third and incisal areas is recommended.
Dentin Exposure on the Margin
In the majority of cases, the placement of the gingival margins for the ceramic veneers is open to subjective criteria. However, there will be some situations where subgingival margins are unavoidable, such as in the case of caries or old fillings that extend under the gingiva.
Patches of dentin exposure are no longer a problem during the preparation as long as the margins are kept on the enamel. However, in most of the abnormal situations, such as extensive caries lesions in the gingival areas, placement of the subgingival margin can go as deep as to be placed on the dentin. Therefore, in order to stop, or minimize the possible marginal leakage, the dentist should very carefully identify the condition of the existing dentin. Thus, obtaining a successful bond to dentin with a perfect marginal seal that will not exhibit discoloration has become a much larger problem that has occupied many researchers over the past four decades.

Islam Zakzouk
DSefa is a blog that's dedicated to bringing you high quality health, lifestyle tutorial and resources on different categories. It's main forus on user experience.














It is quite interesting to see the whole process step by step
ReplyDeleteDoc's Dental
I am constantly surprised by the amount of information accessible on this subject. What you presented was well researched and well written to get your stand on this over to all your readers. Thanks a lot my dear.Movers and packers in Bur Dubai
ReplyDeleteThank you for your addition to this website's extremely amazing information. wordpress website development toronto
ReplyDeleteThank you so much for sharing. Your content was very helpful. You are a marvelous writer. Good work! Custom Optical Coatings.
ReplyDeleteYou are writing is always fabulous. This is third time I’ve read your blog and I find the information very useful. semiconductor and dicing MEMS wafers.
ReplyDeleteI’d like to thank you for writing on this topic. The information you provided was very useful. I will visit again in the near future. Ceramic CNC Machining Services.
ReplyDeleteTrue day, you did an extremely good job. Absolutely, i'll test it out and tell my friends approximately it.
ReplyDeleteThey may genuinely advantage something from this website. Natural Remedies for Dandruff and Itchy Scalp
Thank you so much for sharing. Your content was very helpful. You are a marvelous writer. Good work! Ceramic Substrates and Technical Ceramics.
ReplyDelete