Principles of crown preparation .. Part 2
Biological principles
Preservation of tooth structure
In addition to replacing the lost tooth structure, a restoration must preserve the remaining tooth structure. Preservation of tooth structure in some cases may require that limited amounts of sound tooth structure be removed to prevent subsequent uncontrolled loss of larger quantities of tooth structure. The reaction of the pulp tissue to the tooth preparation is the subject of constant concern during the restorative treatment because it is the only tissue that is located in a chamber that provides mechanical and biological protection.

The proper treatment to repair the tooth can cause damage to the dental pulp. Preparation at high speed is less harmful to the pulp than preparation at low speed due to the decrease of vibration and heat generation, but even when air/water spray is used to cool the area, some degree of pulp irritation will occur. The thickness of the dentin remaining after tooth preparation has been shown to be a critical factor in protecting the pulp from the aggression caused by the preparation. Studies consider a range of 1 to 2 mm of remaining dentin to be sufficient to prevent damage to the pulp. During the preparation for a full crown placement, about 30,000 to 40,000 tubules per mm2 of dentin are exposed. During preparation, worn diamond burs require more pressure from the clinician. This excessive pressure generates more heat on the tooth surface and may cause pulp damage. The pulp tissue should not undergo temperature increases of greater than 5°C, since this could lead to inflammatory reactions and even irreversible damage to the pulp. A temperature increase of 5.6°C in the dental pulp can result in a 15% incidence of necrosis, especially in less voluminous dental elements where pulp necrosis occurs more frequently.
Preservation of the periodontium
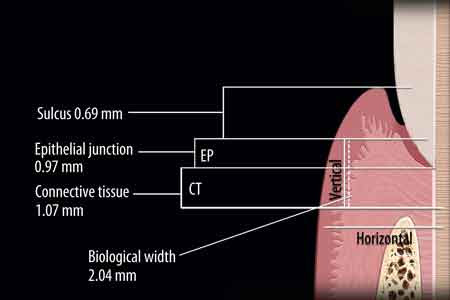
The periodontium forms the basis for esthetics, function, and comfort of the dentition. A healthy periodontium is a prerequisite for all prosthetic rehabilitations. With regard to the interaction of restorations to the periodontium, the most important region is that portion between the crestal bone and the cervical margin of the restoration. In this region, the biological components responsible for the maintenance of periodontal homeostasis are inserted. The connective insertion and the junctional epithelium together compose the biological width, defined as the height of the gingival tissue to the tooth inserted coronally to the bone crest.
When the biological width is invaded and consequently the dentogingival attachment is compromised whether, by pathological (e.g. carious lesion), traumatic (e.g. fractures), or iatrogenic processes (e.g. inappropriate placement of the preparation margins), there is a disruption of the organic seal allowing bacteria and their byproducts to reach the underlying connective tissue which can result in inflammation.
Since the biological width is violated, the body itself is responsible for promoting resorption of the bone crest to allow apical migration of its components. Of course the tissues's response to aggression is different for each individual, but usually it is expressed via gingival recession or periodontal pocket formation. Recession is more common in regions where the alveolar bone plate is thin and sharp, while pockets are usually formed in regions of dense bone and thick gingiva. It should be emphasized that the early diagnosis of the invasion of the biological width is critical - small localized changes can indicate early and easily manageable problems. To avoid this harmful process, a periodontal surgical procedure should be carried out to increase the clinical crown, move the alveolar crest apically, and correct the position of the restoration margin.
Cervical termination of the preparation
To control biofilm, the restoration margins of the preparation must have regular ends and be positioned in areas with better access. This leads to a better periodontal outcome. It is essential that the edges are sharp and well defined in all indirect restorations. It is also important that the termination provides sufficient thickness that favors the stratification of ceramics. When these conditions are not met, the impression does not clearly define the preparation margins and therefore there is a risk that the restoration remains poorly adapted or presents overcontouring that contributes to the development of gingival inflammation and possible attachment loss due to the increased likelihood of biofilm retention, or subcontouring that can lead to increased food impaction and cause damage to the periodontal tissues, leading to the formation of periodontal pockets.



Although the restoration margin should preferably be placed supragingivally (A), for esthetic reasons it is sometimes placed gingivally/equigingivally (B) or subgingivally (C).
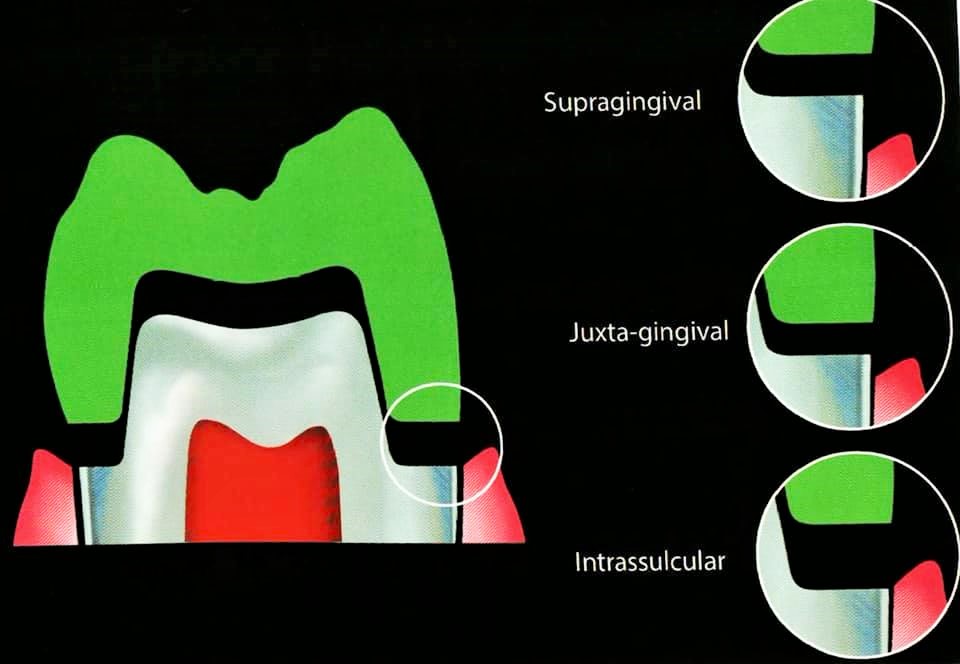
Ideally, the end should be maintained as far as possible from the gingiva (supragingival), since this is the most favorable situation for the periodontium, not only throughout the prosthetic treatment, but also for the maintenance and longevity of the restoration. However, for several reasons - aesthetics, retention, the extent of preexisting lesions - the preparation can be extended to the gingival level (juxtagingival / equigingival) or slightly inside the sulcus (intrasulcular / subgingival ). These three alternatives satisfy the biological distances and are well tolerated by the periodontium.
Deeper locations of the restoration margins into the gingival sulcus result in more inflammatory responses. Some authors have considered the presence of restorations with subgingival margins as one of the main risk factors for periodontitis. Of course, whatever the position of the finish line, the procedures of preparation and cementation should be as atraumatic as possible (eg, it is useless to have an equigingival termination if excess cement is left after cementation, which could compromise the periodontal health).
Whenever possible, the cervical termination should be scribed at first, following the anatomical contour of the region. This is a safe way to establish the width of the cervical reduction and guide the axial preparation. Gingival displacement is another alternative that can be employed to minimize the risk of damaging the epithelium during the preparation. An adequate reduction of the tooth should always be pursued during preparation to create enough space for the placement of the future restoration.
Alternatives that help to preserve the periodontium during tooth preparatio; gingival groove and retraction cord.


If insufficient tooth structure has been removed, the future restoration will be overcontoured. Overcontouring of the restoration margin is a contributing factor to the development of gingival inflammation and possible periodontal attachment loss due to the increased potential of biofilm retention. Biofilm retention can also occur in cases of poor-contour restorations. Undercontouring can lead to increased food impaction and cause damage to the periodontal tissues, leading to the formation of periodontal pockets.


There are several guidelines for predicting the post restorative gingival margin levels and the periodontal health after preparation, gingival retraction, and impression-taking. These guidelines should be considered during the diagnostic phase and before the restorative appointment because they can provide the patient with a stable and healthy periodontium after preparation, impression-taking, and placement of the restoration. Measurements on the facial and interproximal regions of the unprepared tooth can provide predictable categorization. These osseous crest positions can be divided into three categories: normal, low, and high.

For a normal crest position, these two measurements for anterior teeth should be approximately 3 mm on the facial and 4 mm on the interproximal when adjacent teeth are present, and this relationship occurs in approximately 85% of patients.
When the depth of the osseous crest to the gingival margin is greater than these measurements, it is considered to be a low crest position, which occurs in approximately 13% of patients.
If the depths are less than these measurements, it is considered to be a high crest position, which occurs in 2% of patients.
In a normal osseous crest position, the gingival complex will return to a normal crest relationship after tissue manipulation and impression-taking. However, in a high crest relationship, traumatic manipulation and placement of subgingival preparation margins will position the definitive restoration too close to the osseous crest, creating a violation in biologic width. The low crest position with a thin biotype is considered the most unstable clinical situation and can result in the most variation in the final gingival position.
For optimal restorative results, the low and high osseous crest positions should be identified in the diagnostic phase and corrected through osseous and/or orthodontic treatment before restorative treatment.
In clinical situations where adjunctive therapy is not planned, careful and gentle manipulation during the impression-taking process is critical. During gingival displacement, therefore, the size and number of retraction cords should be modified according to the osseous crest position and tissue biotype. It is suggested to use a single-cord technique on high and low crest positions and a double-cord technique on normal crest positions.
When preparing a crown, mechanical, biological, and esthetic principles must be respected. These principles act in a concomitant way in the search for and implementation of the preparation finish line. This finish line is primarily responsible for the marginal integrity of the restoration, being closely related to its cervical adaptation. A qualitative adaptation of these restorations reduces the biofilm accumulation and the chance of periodontal tissue damage, thus extending the longevity of the prosthetic treatment. The preservation of the marginal integrity is directly related to the most critical stage of the preparation, which is the preparation of the cervical finish. This may have different configurations, depending on the properties of the materials to be used in the manufacturing of the crown.
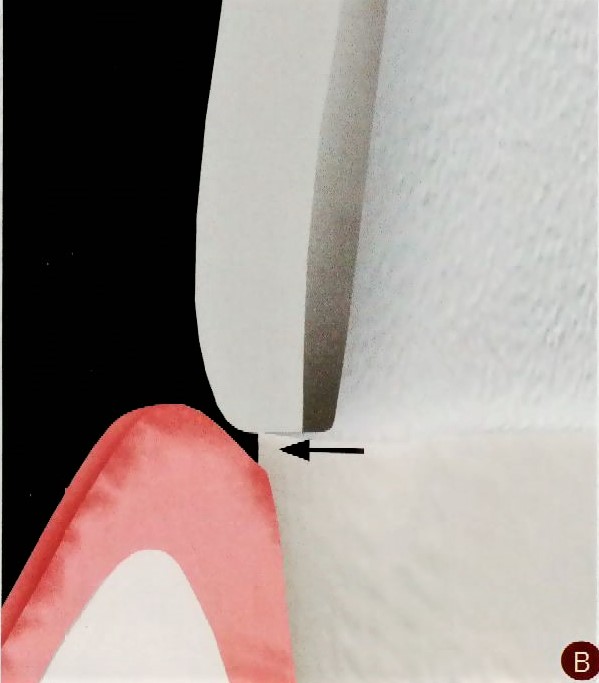
Maintaining marginal integrity is directly related to the level of marginal adaptation defined by the space between the inner surface of the prepared tooth and the restoration.
A marginal gap ranging from 10-500 Mm with average values between 50 and 100 Mm has been defined as acceptable. Marginal openings from 50 to 120 Mm are considered clinically acceptable in terms of longevity. For CAD/CAM restorations, the generally acceptable marginal gaps range from 50 to 100 Mm.

Proper positioning of the restoration margin favors maintaining marginal integrity.
The cervical finish line is usually the last step of a crown preparation. To obtain greater smoothness and uniformity in reduction, the use of a rotating device with a minimum pressure, maximum cooling, and new diamond burs is recommended. The correct indication and execution of the finish line contributes significantly to the preservation of health and periodontal integrity. Selecting the type of finish line depends on local and esthetic factors, as well as on the chosen restorative material.
Esthetic principles
When rehabilitation is required in the esthetic zone, increased attention should be paid to the connection between the gingiva and prosthetic parts. This connection is the weak point and the place where patients most often notice that “the tooth is a fake”. The composition of a smile that is considered beautiful, healthy, and attractive involves a balance between the shape and symmetry of the teeth, lips, and gums, including the way in which these elements relate to and harmonize with the patient’s face. Importantly, all of these references should be sought in conjunction with functional principles of occlusion, incisal guidance, canine guidance, overbite, and overjet.
It is necessary that the available space, defined through the reduction with diamond points, is compatible with the restorative system to be used.
Because different biomaterials require variations in thickness for strength, the preparation dimensions for full-coverage restorations can vary. All-ceramic crowns can be fabricated from one ceramic (eg, pressed or machined by CAD/CAM), or a combination of a ceramic coping and a reinforced veneering ceramic, with improved aesthetic features. These copings may be fabricated with different materials - lithium disilicate, alumina, zirconium dioxide - and for different systems, such as e.max (Ivoclar Vivadent), Procera (Nobel Biocare), lnCeram (VITA), and Lava (3M ESPE). Some of these systems allow for obtaining high strength ceramic infrastructures, even in small thicknesses (0.3 mm) facilitating the obtaining of less invasive preparations, without aesthetic impairment.
Clearly, the degree of translucency/opacity of the coping - a critical aspect in defining the aesthetic potential of each restorative system- varies significantly from one material to another. It should be stressed that the thickness of the coping, as well as its degree of translucency/ opacity, must be defined according to the color of the substrate to ensure perfect masking of its shade.
The darker the underlying tooth structure, the less translucent and/or thicker the coping should be.
Islam Zakzouk
DSefa is a blog that's dedicated to bringing you high quality health, lifestyle tutorial and resources on different categories. It's main forus on user experience.











great topic thwnks alot
ReplyDeleteThanks alot
ReplyDeleteGreat topic thanks alote dear dr eslam
ReplyDelete