Veneers are partial extracoronal restorations usually indicated for anterior esthetic rehabilitations. The main purpose of a veneer is to cover the labial-proximal surfaces and potentially the incisal border of the anterior teeth in an attempt to correct color discrepancies, shape, texture, function, and position of the elements in the dental arch. There are several preparation designs for ceramic veneers, which vary according to the extent of the preparation. The use of different preparation techniques is dependent on several factors: the amount of remaining tooth structure, presence of previous restorations, length of the clinical crown, and presence of endodontic treatment.
Preparations for laminate veneers do, in fact, require great stringency and a great deal of training, as no rectification can be made once the procedure is completed. Experience is required for mastery of 0.3-0.5 mm reductions.
Enamel Vs Dentin
Tooth preparation for the laminate veneers is exacting. Using magnification loupes to facilitate careful preparation is tremendously helpful for accomplishing this step. It also helps to preserve as much enamel as possible as the bond strength of porcelain bonded to enamel is still superior when compared with the bond strength of porcelain bonded to dentin.
The more the bonding surfaces were located in dentin, the lower the success rate..
This could be explained by the difference in the elastic modulus between the substrate and the ceramic. The lower this ratio, the better the fracture resistance. This explains why bonding to enamel (70 GPa) is preferable to dentin (18 GPa) because the difference in the elastic modulus is lower with ceramic (between 65 GPa for feldspathic and 95 GPa for IPS e.max).
Dentistry
To ensure the bond strength of the resin composite to the tooth surface it is necessary to reduce the enamel. Due to its poor retention capacity, the aprismatic top surface of mature teeth that have not been prepared must be removed, or at least roughened. Careful attention is of the utmost importance in order to obtain successful results and solid bonding. However, Rigidity in the tooth is due to the amount of enamel thickness, and thus,
The more enamel that is removed, the more the tooth flexes.
As the anatomy and the shade of the restoration are directly affected by the preparation design, very precise planning is necessary. The ceramic material allows for the reproduction of natural light transmission (i.e. refraction, reflection, translucency) and an esthetic result can be hindered by insufficient tooth preparation in relation to the soft tissue parameters and the restoration.
Enamel removal
The shape of the preparations also influences the appearance and longevity of a restoration. In order to manipulate light and to establish a depth of translucency and space for the incisal effects is desired.
Without reduction, the teeth will be larger and more labially positioned (in lingually inclined teeth, this may be an advantage). Failure to remove proximal enamel can result in the finish line placed too far labially and encroachment on the embrasure areas, resulting in exposure of unsightly porcelain margins that may be difficult to finish. Proceeding without preparation will lead to not only distinct overcontouring at cervical and proximal tooth surfaces, but also to higher clinical failure rates as a result of gingival inflammation and secondary caries due to an increase in microbial plaque accumulation.
The continuing evolution of bonding processes to dental structures makes possible the implementation of more conservative restorative techniques and enables the use of minimally invasive preparations.
In teeth with slight or no discoloration, for example, ceramic veneers with thicknesses ranging from 0.3 to 0.7 mm may be used. Extremely thin ceramic veneers emerged, requiring minimal tooth reduction that is limited to merely smoothing sharp angles and eliminating undercuts. Teeth indicated to receive this type of restoration usually have favorable characteristics such as a good insertion axis and adequate space for the restoration. These preparations have very specific indications, where reshaping or correction of tooth volume is necessary by adding material.
NB. It should be noted that ceramic veneers are of limited use in situations requiring major correction.
When to consider reduction?
- Remove convexities and provide a path for insertion in those situations where either the incisal or the interproximal areas are to be included in the veneer.
- Provide space for adequate opaquing or heavier coloring like in cases of a dark substrate.
- Provide a definite seat to help to position the veneer during placement.
- Prepare a receptive enamel surface for etching and bonding the veneer.
- Allow for a smoother transition from the veneer to the tooth surface, enabling the patient to more easily keep it plaque‐free.
Contraindications to reduction:
- The size of the pulp. If young individuals or others with large pulps require laminating, consider an alternative to enamel reduction, especially if there is any indication of irreversible sensitivity by reducing the thickness of the enamel.
- The patient’s psychological state and feelings about tooth reduction or veneers. If the patient is apprehensive and unsure, then it is wise to do no reduction. Then if the patient becomes dissatisfied with the veneer or the slightly overbuilt look, the option will be removing the porcelain veneer and repolishing the enamel, thus returning the patient to a semblance of their pre‐veneer state.
As a general principle, the enamel should be reduced just as much as necessary to facilitate the placement of an esthetic restoration. Ideally, one would like to remove the same amount of enamel that will eventually be replaced by the veneer and bonding composite resin. Decisions about reduction need to take into account the relative position of the tooth in the arch. For example, in treating a crowded or rotated tooth or a tooth in a labial version, it may be advantageous to first bring the offending tooth into alignment with the rest of the arch by reducing its labial contour through cosmetic contouring. Thus, The use of mock‐ups, followed by a wax model, esthetic pre‐evaluative temporaries, and silicone index, provides the best esthetic, phonetic, and functional assessment of necessary tooth preparation for veneers.
Veneers preparations
Preparations for ceramic veneers have undergone many changes and advances. The preparation shape can be influenced by tooth shape, location and orientation in the arch, tooth anatomy, occlusal function, mechanical forces, quantity and quality of the remaining tooth structure and anticipated final restorative dimension. By using these clinical considerations, modifications in the preparation shapes may be varied and find a multitude of shapes, being guided by the pre-existing defect or depending on the anticipated dimension of the final restoration and the substrate shade.
The goals of preparation:
- To create enough space for the ceramic material
- To maintain as much enamel as possible.
- Definite finish line for the technician.
- Smooth preparation without sharp line angles.
No prep
This concept has become very popular in recent years due to its commercial attractiveness for patients. However, it is important to highlight the many limitations; esthetically (overhangs) and in terms of its application in the laboratory (ultra-thin veneers) and in the clinic (extremely delicate to bond). Very few clinical situations are in fact eligible for this purely additive concept.
Recently, interdisciplinary care was a pillar of this evolution by fully including orthodontics in the treatment plans. The orthodontic movement would create the necessary thickness (0.5 mm) for the final restorations. As a result, the clinician only had to draw the contours of the preparation without having to reduce the thickness of the tooth unnecessarily. This principle must according to logic, follow the final esthetic plan that was established at the beginning of the treatment. The positioning sought by the orthodontic action must be controlled and the occlusal key based on the wax-up should validate the obtained space. Thus, it is still some sort of debate and can not be applied to all cases but needs precise case selection.
It is worth remembering that the final objective and the thickness of the restorative material should be considered to avoid overcontouring of the restored teeth. Another consideration is the amount of masking required on the dental structure. Several discolorations could require considerable thickness of restorative material and as a result, a more invasive tooth preparation result and to determine the final thickness and morphology of the tooth and of the restoration.
Some of the advantages of this concept in relation to conventional veneers (with preparation) are:
- preservation of sound tooth structure
- reduced clinical time for the impression-taking step
- elimination of the provisional step
- bonding exclusively to enamel.
- the meticulous and thorough manufacturing of the laboratory step
- increased risk of fracture during the various steps of the process (laboratory, try-in and cementation) due to thinness of the veneer,
- critical cementation process and thoughtful maintenance therapies, concerning the maintenance of the aesthetic result,
- these veneers do not involve the areas of dynamic visibility, which will become visibly present with the natural darkening of the dental substrate.
Stay tuned for upcoming posts discussing this topic in much more details ..
Extensive preparation
The tooth is at greater risk when the potential treatment requires extensive preparation. Because this can may to:
- Biologic irritation to the pulp
- Adhesion impairment.
In this case the preparation is extended to the proximal sufraces and overlap the free edge in what was commonly referred to as "palatal overlap". Although the preparation is slightly extended to the lingual surface increasing the total surface of enamel for bonding, at the same time also creates the correct path for insertion during the try-in and cementation, this type of veneers preparation can be considered extensive.
Despite the good biologic integration and the quality of cementation, the palatal overlap led to mechanical complications, related to a repositioning of the palatal margin in the area of greatest functional stress; the cingulum. This type of preparation therefore had two major drawbacks:
- Frequent debonding of the restoration due to functional overload during occlusion.
- This invasive preparation resulted in excessive dentin exposure.
Palatal concavity that provides the incisor with its sharp incisal edge and cutting ability, proved to be an area of stress concentration. Logically, the preparation should preferably not finish at the concavity but rather it should be placed either above the concavity or below on the smooth convex area of the cingulum so that they will be subject to low tensile forces. Placement of the lingual finish line for a laminate veneer will also depend on the thickness of the tooth and the patient's occlusion.
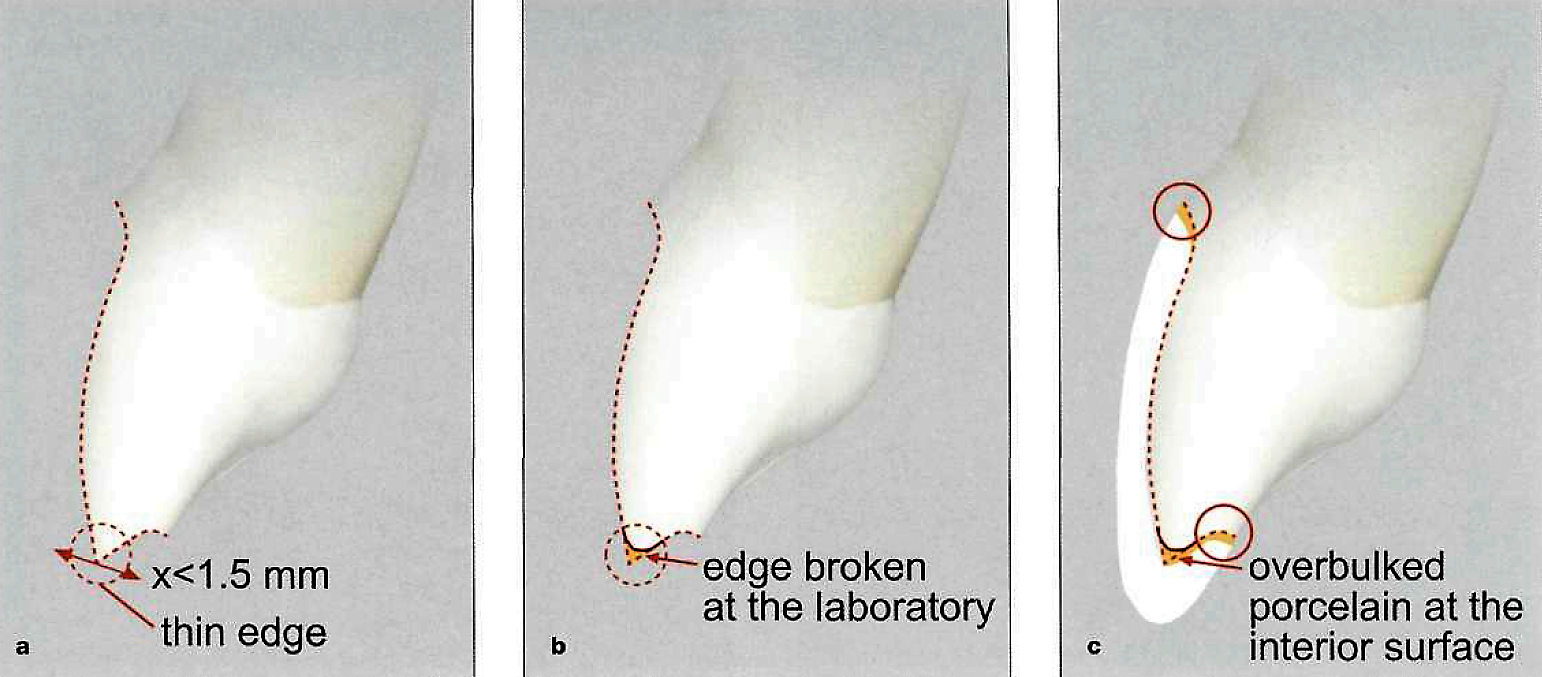
If the preparation needs to be extended palatally over the incisal edge, the remaining part towards the incisal should have enough thickness to prevent breakage. When the teeth are thinner than 1.5 mm labiolingually at the incisal third, reducing the labial and the lingual surfaces incisally by 0.5 mm, the preparation leaves us with a thin sliver tooth structure that cannot be rounded off and is susceptible to breaking. These areas are sometimes kept so thin that they even break at the laboratory while the technician tries to take the refractory dies out of the impression, or at the time of the provisional's removal. This situation may cause another serious problem if the tip of the stone model coincides with the very thin portion and is broken during the lab procedures, resulting in a ceramic veneer with extra porcelain in that area.
When that veneer is seated on the tooth, care must be taken to avoid mistakes due to the overbulked interior surface of the incisal edge which will make it impossible to seat the veneer properly and result in an inaccurate fit at the cervical margin.
The authors do not advocate performing this termination because the biological cost is higher. The creation of an insertion path facilitates the cementation step, however promotes a higher volume of wear, particularly in the proximal regions to eliminate retentions. Hence, straight-type incisal terminations are preferably chosen when reduction is necessary because it advocates a passive fit in the labial-palatal direction without a deliberate insertion axis, greater preservation of tooth structure, and lends absolute confidence in the bonding mechanisms.
Conventional preparation
It is fully explained in this link .... click this link
Guided preparation
The most recent and important. It is fully explained in this link ....
"stay tuned"
To get the PDF file click this link
Ceramic Veneers Preparation

Islam Zakzouk
DSefa is a blog that's dedicated to bringing you high quality health, lifestyle tutorial and resources on different categories. It's main forus on user experience.
















thanks alot for your efforts.
ReplyDeleteThanks for your post. I’ve been thinking about writing a very comparable post over the last couple of weeks, I’ll probably keep it short and sweet and link to this instead if thats cool. Thanks. Invisalign Milton Keynes
ReplyDeleteMy allhe bless you i will read it and i will re thank y again
ReplyDeleteYou are the best , greeting from morocco
ReplyDeleteYou are the best , greeting from morocco
ReplyDeleteThanks for ur effort👌
ReplyDeleteGreat work
ReplyDeleteGreat information
Thanks
شكرا جزيلا يا دكتور 💕
ReplyDeleteتسلم يا دكتورنا
ReplyDeleteThanks doctor
ReplyDeleteThanks doctor
ReplyDeleteThank you doc, This is one comprehensive post I must say
ReplyDeleteDoc's Dental
Excellent article. Very interesting to read. I really love to read such a nice article. Thanks! keep rocking. Movers and packers in Bur Dubai
ReplyDeleteyour way of explaining makes it look very easy, thank you for sharing such knoledge
ReplyDeleteI’ve been reading numerous articles on this topic but found this one uniquely written. Thanks. Customize Silicon Wafers From Valley Design.
ReplyDelete